Herpes
- Ask the DOC
Rockaway Stuff
- 0
- 3 minutes read

By Peter Galvin, MD
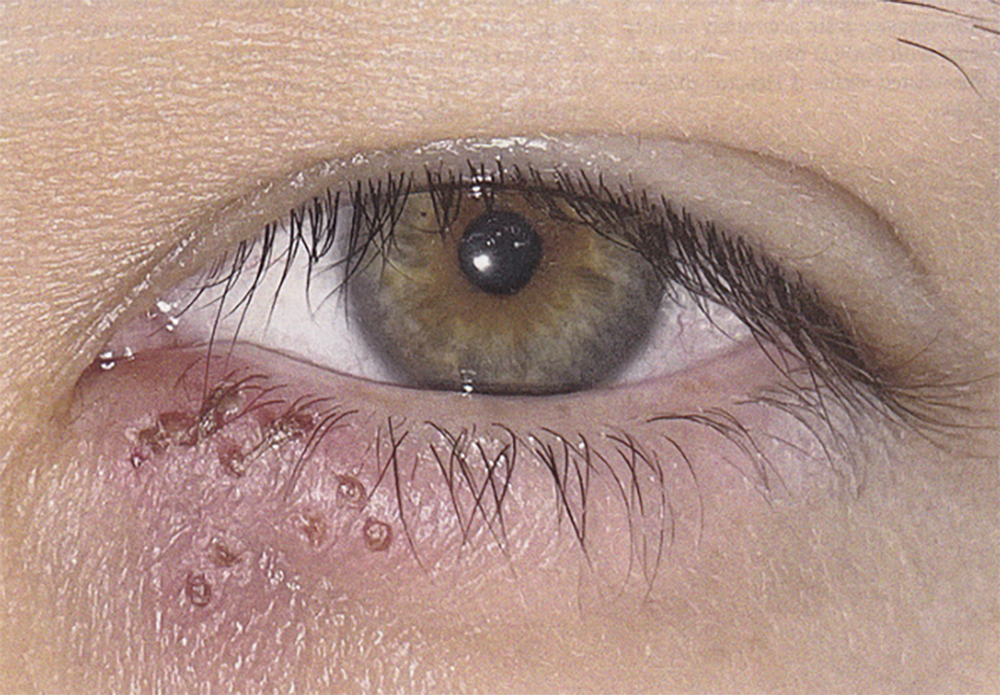
A healthy 30-year-old man presented to the ophthalmology clinic in Alicante, Spain with a three-day history of recurrent, painful bumps on his left lower eyelid. He reported having annual recurrences of similar lesions at the same site since adolescence and that the episodes were often triggered by psychological stress or sun exposure. Each episode had lasted three to five days and resolved spontaneously. He had not previously sought care for this owing to the mild and self-limited nature of the symptoms. On physical examination, clustered erosions and ulcers were observed on an erythematous (red) base on the medial (inner) aspect of the left lower eyelid margin (see photo). Visual acuity and slit-lamp examination were normal.
Polymerase-chain-reaction assay of a swab specimen from a lesion was positive for herpes simplex virus (HSV) type 1. A diagnosis of HSV blepharitis (eye lid infection) – with reactivation within the sensory territory of the infraorbital branch of the maxillary division of the trigeminal nerve – was made. Although HSV eye infections may involve only the eyelid, prompt evaluation is recommended to be sure there is no ocular involvement as ocular involvement can cause blindness. If you are thinking this is like shingles, you would be correct.
There are two types of herpes simplex, types 1 and 2. Historically, HSV 1 caused inflammation of the mucous membranes of the mouth, lips (“cold sore”), and nose but, unlike type 2, did not cause genital disease. That is no longer the case. Well over 70% of the world’s population has HSV 1. Once acquired, the herpes virus, and this includes the herpes zoster (shingles virus), never leaves the body. The virus “hides” from the immune system by getting into the cell bodies of neurons (nerves) where the immune system cannot detect it. Occasionally, the virus reactivates, causing skin or mucous membrane lesions within the distribution of the nerve, which sheds the virus. This is when the person becomes contagious. The viruses cannot be passed on by skin touching but can be passed to another person by contact with mucous membranes, for example kissing and unprotected oral and genital sex.
Currently, there is no affective method to remove herpes viruses from the body. The flare-ups can be treated with antiviral medications which lessen symptoms but do not eradicate the virus. While HSV 1 flare-ups are associated with stress and sunlight exposure as in this case, the cause of flare-ups of HSV 2 and herpes zoster is mostly unknown. The patient in this case was given a 5-day course of oral acyclovir and his symptoms resolved. At a six-month follow-up, his eye was normal.
Please direct questions or comments to editor@rockawaytimes.com


