Blocked
- Ask the DOC
Rockaway Stuff
- 0
- 3 minutes read

By Peter Galvin, MD
Today’s case study comes from Weill Cornell Medicine in Manhattan. But before I get to the case, I would like to lay some groundwork. The heart has its own internal pacemaker, known as the sinoatrial node, or SA node. It is located in the heart’s upper chamber, the atrium. When the SA node fires, it generates an electrical impulse that causes the atria to contract, pushing blood into the lower chamber, or ventricles. The SA node’s impulse travels down a conduction system into the ventricles, causing them to contract after a slight delay. This electrical activity can be tracked by an electrocardiogram, or ECG. The SA node’s impulse and atrial contraction causes a small, usually upward, bump, called the P wave. This is followed by a narrow spike, often both upward and downward, caused by the contraction of the ventricles, called the QRS complex. Finally, a larger, broader upward bump, called the T wave, is caused by the electrical repolarization, or resetting, of the ventricles.
A 70-year-old man with hypertension and coronary artery disease (CAD) presented to the ER with a several-hour history of shortness of breath and a slow heart rate. On the day he came to the ER, his commercial mattress – which included a ballistocardiographic monitoring feature – had alerted him that his average heart rate the night before during sleep (42 beats per minute [bpm]) was lower than his usual (78 bpm). Using his smartwatch and home blood pressure machine, the patient had confirmed ongoing bradycardia (slow heart rate). After noting new shortness of breath with exertion (dyspnea), he called his primary care doctor who advised him to go to the ER.
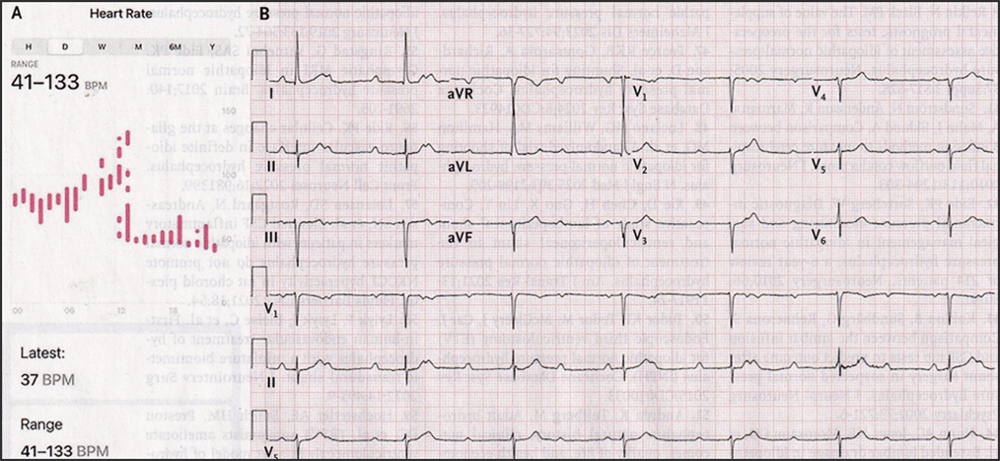
In the ER, his heart rate was 40 bpm, and his blood pressure was 127/64. Physical examination was remarkable only for bradycardia. A review of the heart-rate trend on his smartwatch showed a sudden decrease in the heart rate at 2 p.m. the day before presentation (Panel A). An ECG showed complete heart block with a junctional escape rhythm (Panel B). Complete heart block can most easily be seen on the 5th line down labeled “II.” The small bumps, P waves, march across the strip with no relation to the QRS complex. As noted above, each heartbeat should begin with a P wave, followed by a QRS complex, and lastly a T wave. That is not the case here. What has happened is that the impulse from the SA node is not reaching the ventricles, causing the ventricles’ accessory pacemaker to trigger contraction of the ventricles. This is called a junctional escape rhythm.
The most common cause of complete heart block is ischemic (insufficient blood flow) heart disease, which this patient had. Lack of oxygen damages the tissues containing the SA node’s conduction system. The patient had a dual-chamber pacemaker placed, and his symptoms abated. Unlike a standard pacemaker, which generates an electrical impulse to cause the heart to contract, a dual-chamber pacemaker detects the impulse from the SA node and, after an appropriate delay, triggers the ventricles to contract. What amazes me about this case is the technology, I mean I know about smart watches but now we have “smart” beds too? Who knew?
Please direct questions and comments to editor@rockawaytimes.com