Collapse
- NEWS
Rockaway Stuff
- 0
- 2 minutes read

By Peter Galvin, MD
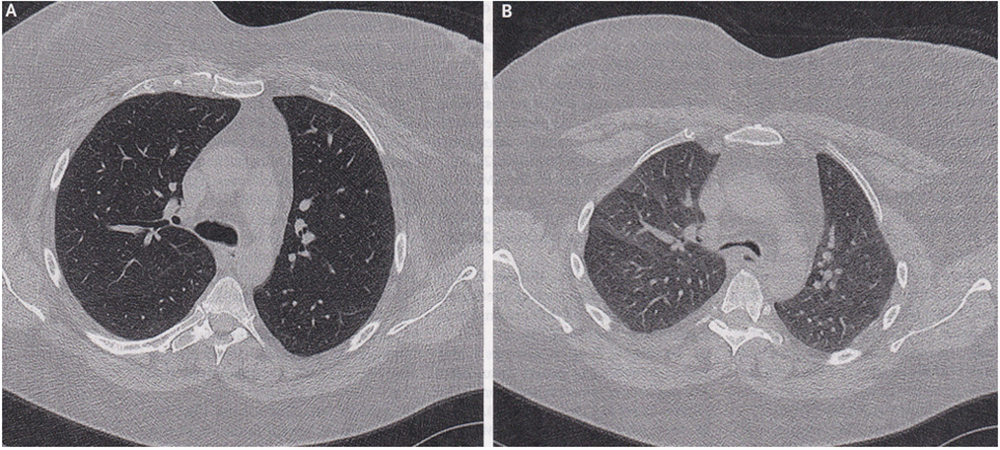
A 50-year-old woman with a history of asthma, obstructive sleep apnea, and obesity was referred to the pulmonary clinic at the University of Iowa Hospitals and Clinics in Iowa City with a one-month history of worsening shortness of breath and dry cough despite maximum treatment for asthma. On physical examination, expiratory stridor (a high-pitched noise usually caused by airway obstruction) and reduced breath sounds throughout the chest were noted. Dynamic computerized tomography (CT scan) of the chest – a study of the airway during different phases of respiration – showed anterior bowing of the posterior wall of the intrathoracic (in the chest) trachea and mainstem bronchi on expiration, with more than 70% collapse as compared to inspiration (Panel A, inspiration; Panel B, expiration, airway in the center of both images). A diagnosis of expiratory central airway collapse – a condition characterized by pathologic collapse of the central airways during expiration, resulting in dynamic outflow obstruction – was made.
Expiratory central airway collapse is associated with common conditions such as asthma, obesity, and chronic obstructive pulmonary disease (COPD). It is important to consider this diagnosis in patients with persistent respiratory symptoms despite intensive treatment of known coexisting illnesses. After a one-week hospital stay for pulmonary clearance and initiation of nocturnal positive airway pressure (CPAP), the patient’s symptoms abated, albeit temporarily. She was then referred to a multidisciplinary program for complex airway management. She wound up undergoing robotic-assisted mesh tracheobronchoplasty (essentially a tracheal stent), after which her symptoms improved substantially and for the long term.
Please direct questions and comments to editor@rockawaytimes.com


