What a Pity…
- Ask the DOC
Rockaway Stuff
- 0
- 2 minutes read

By Peter Galvin, MD
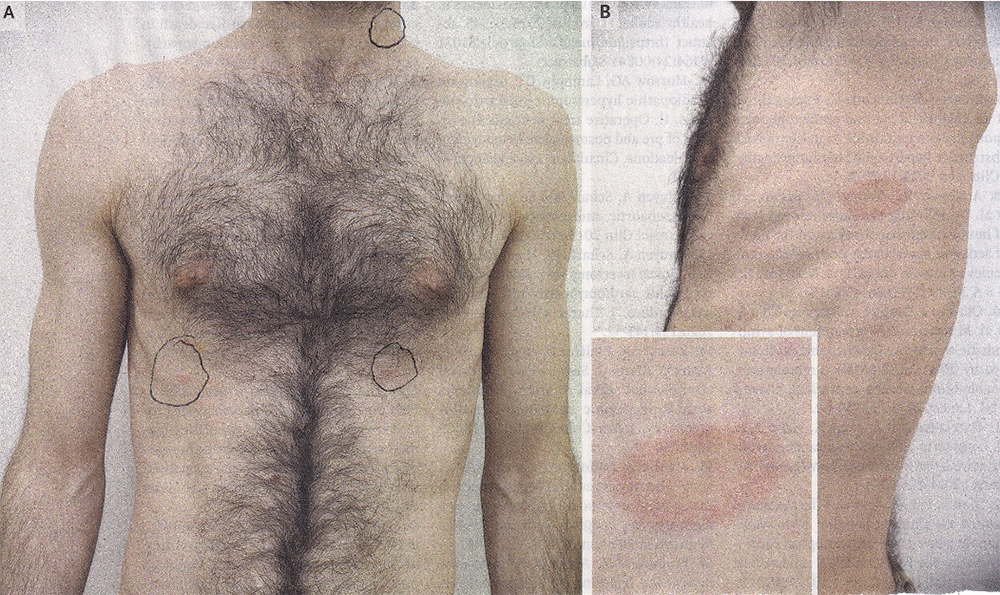
A previously healthy 42-year-old man presented to the dermatology clinic in Athens, Greece with a 20-day history of an expanding, asymptomatic rash on his trunk. The first lesion had been a red spot on the patient’s left side. Ten days after that spot first appeared, smaller lesions had started developing elsewhere. The patient denied having a prior viral infection (prodrome). Physical examination was notable for multiple 1-to 4-cm ovoid, erythematous (red), papulosquamous plaques on the chest, neck, and proximal (upper) arms (Panel A). The initial lesion – an 8.5-by-5.5-cm patch with central clearing and peripheral (outer) scaling – was seen on the midaxillary (armpit) line on the left side (Panel B and inset). On the basis of finding a “herald” patch, a diagnosis of pityriasis rosea was made.
Pityriasis rosea is a self-limited disorder that commonly affects children, adolescents, and young adults, usually between the age of 10 to 35 years. It was first described in 1798. Often, but not always, the lesions align along the cleavage lines of the skin, forming a “Christmas tree” pattern. The cause is unclear, although some studies have reported that up to 70% of patients had a recent, prior viral upper respiratory infection. Pityriasis rosea is not thought to be associated with bacterial or fungal organisms, although it may be related to reactivation of human herpes virus 6 or 7. Most cases are asymptomatic, but some studies have described flu-like symptoms. In some cases, the lesions are itchy.
Outside of a dermatology practice, pityriasis rosea is often misdiagnosed as Lyme disease, ringworm, psoriasis, eczema, or a viral rash (exanthem). There is no specific treatment, although sometimes a topical steroid cream is prescribed if itching is present. Exposure to sunlight often hastens its disappearance, so occasionally UV light treatment is recommended. In most cases, the rash resolves by itself over a period of a few weeks to months. In this case, the patient was reassured regarding the benign nature of the rash, and a month later the rash had disappeared.
Please direct questions and comments to editor@rockawaytimes.com


