You’re All Heart
- NEWS
Rockaway Stuff
- 0
- 3 minutes read

By Peter Galvin, MD
Coronary artery plaque is the buildup of deposits that may include cholesterol and calcium on the inner walls of the arteries of the heart (coronary arteries). These deposits can narrow or block these arteries, decreasing blood flow to the heart, which may cause a heart attack. The standard non-invasive method to detect coronary artery calcium is a gated cardiac computed tomography (CT) scan, which times the acquisition of images with the patient’s EKG to improve image quality. The coronary artery calcium score, which is calculated by adding up the amount of calcium detected in each of the coronary arteries, ranges from 0 (no calcified plaque) to more than 1000 Agatston units (extensive plaque). Calcium can also be detected on non-gated CT chest scans but is less precise and is reported as absent, mild, moderate, or severe.
Plaque increases with age and is more common in men than women of all ages. Among those younger than 55 years, more than half without known coronary artery disease will have no detectable coronary artery calcium. However, among those aged 80 years and older, more than 80% have some detectable calcium. The coronary artery calcium score strongly predicts future atherosclerotic cardiovascular disease (ASCVD) events, which include heart attack, stroke, resuscitated cardiac arrest, and cardiac death. Those with coronary calcium scores of greater than 300 Agatston units have ASCVD event rates of about 13% to 26% over 10 years compared to 1% to 6% in those with a calcium score of 0.
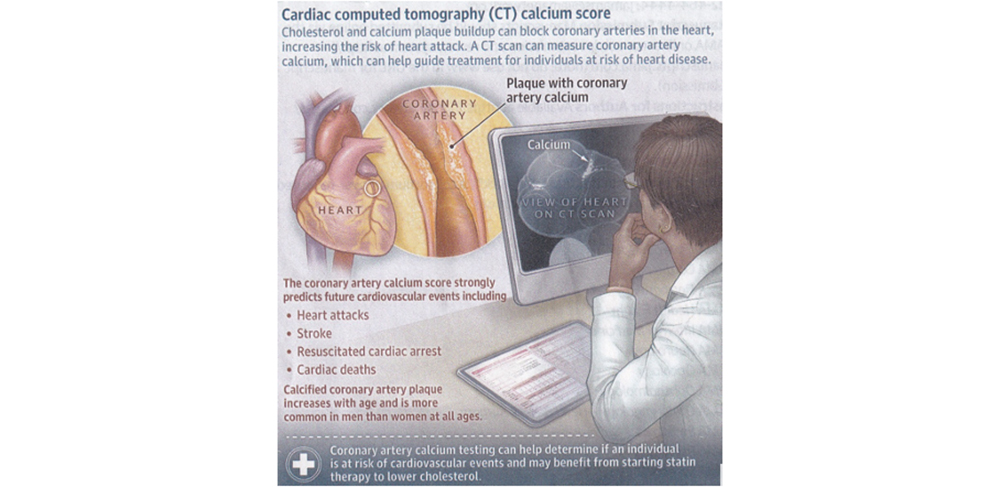
Coronary artery calcium testing can help determine if a person is at risk for ASCVD and may benefit from the use of a cholesterol-lowering medication (statin). Statin therapy is recommended for asymptomatic individuals with a coronary calcium score of 100 Agatston units or higher and may be considered for those with a score of 1 to 99 Agatston units, especially if they are younger than 45 years. Coronary artery calcium testing is not recommended for people with known ASCVD as well as people with certain conditions such as diabetes, current smoking, and familial hyperlipidemia, because for them statin therapy would be recommended regardless of calcium score. People with a coronary calcium score on gated cardiac CT who are placed on a statin should not undergo repeat testing because a change in their calcium score would not alter treatment. For those with an initial calcium score of 0, repeat testing may be considered after five years in those older than 40 years.
Coronary artery calcium testing for asymptomatic individuals is not covered by Medicare or Medicaid and is typically not covered by private insurance as well. Out-of-pocket costs range from about $50 to $400. Coronary artery calcium testing can also lead to increased costs from additional cardiac testing (stress testing, cardiac catheterization) and follow-up testing of incidental findings such as lung nodules or aortic dilation.
For more information go to the website of the American Heart Association at www.heart.org
Please direct questions or comments to editor@rockawaytimes.com


